Session Information
Date: Sunday, November 12, 2023
Title: (0380–0422) RA – Diagnosis, Manifestations, and Outcomes Poster I
Session Type: Poster Session A
Session Time: 9:00AM-11:00AM
Background/Purpose: Routine Assessment of Patient Index Data 3 (RAPID3) is a patient-reported outcome (PRO) that can be used to assess the condition of rheumatoid arthritis (RA) patients using only a questionnaire that can be completed in a short time. In previous reports, RAPID3 could be used as an assessment similar to Disease Activity Score 28 (DAS28), a common disease activity assessment [1]. However, there are unmet needs in which patients have low satisfaction with treatment, even though they are in remission according to disease activity assessments such as DAS28. To investigate the cause of this discrepancy, we decided to conduct a study using RAPID3 as a subjective patient assessment. The aime of this study was to investigate the discrepancy between disease activity and RAPID3 in RA patients.
Methods: The data for this study were obtained from the Tsurumai-Frailty and Locomotive Syndrome of Rheumatoid Arthritis for Globalization (T-FLAG), an observational study involving three centers. Of the 638 RA patients who completed the PRO questionnaire in 2022, 455 patients with a DAS28-CRP of low disease activity (LDA) or remission (REM) were enrolled. Disease activity was assessed using the RAPID3, DAS28-CRP. PRO assessment was performed using PtGA, Health Assessment Questionnaire Disability Index (HAQ-DI), Kihon checklist (KCL), and the 25-question Geriatric Locomotive Function Scale (GLFS-25). RAPID3 categories were compared in two groups: REM/LDA, and medium and high disease activity (MDA/HDA). Cutoff values for each PRO were detected using ROC analysis.
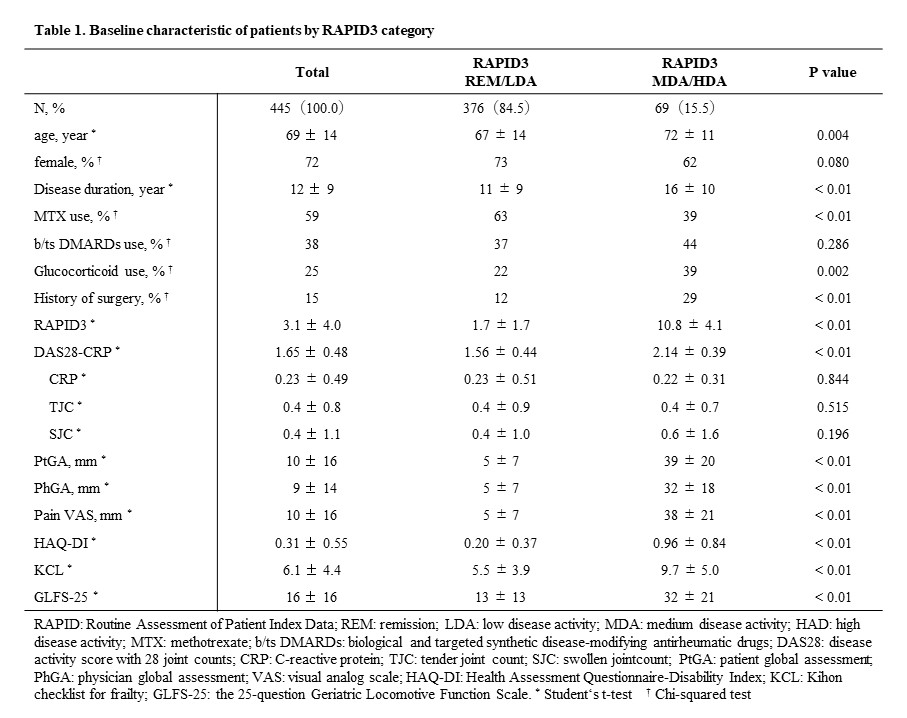
Results: The mean age (± standard deviation) was 69±14, female was 72%, disease duration was 12±9, RAPID3 was 3.1±4.0, DAS28-CRP was 1.65±0.48, HAQ-DI was 0.31±0.55, and KCL was 6.1±4.4. In the disease activity category, 84.5% of patients had RAPID3 and DAS28-CRP in the same category (The disease activity category of RAPID3 was LDA or REM). There were no significant differences in gender, biological and targeted synthetic disease-modifying antirheumatic drugs, C-reactive protein, tender joint count, swollen joint count between the two groups of REM/LDA and MDA/HAD (Table 1). On the other hand, there were significant differences between the two groups in disease duration (11 vs. 16 years), PtGA (5 vs. 39mm), HAQ-DI (0.20 vs. 0.96), KCL (5.5 vs. 9.7), and GLFS-25 (13 vs. 32). The cutoff values for PRO assessment for different disease activity categories of patients were HAQ-DI 0.375 points, KCL 8 points, and GLFS-25 16 points.
Conclusion: In this study of patients with good disease activity control, 84.5% of patients were found to have a concordance between RAPID3 and DAS28 disease activity categories. The discrepancy between DAS28-CRP and RAPID3 may be due to physical dysfunction (HAQ-DI or GLFS-25) or frailty (KCL). Therefore, it is important to achieve clinical remission and improve PRO in RA treatment as an intervention to address unmet needs.
To cite this abstract in AMA style:
Suzuki M, Takahashi N, Sobue Y, Ohashi y, Sato R, Maeda M, Kosugiyama H, Ohno y, terabe k, Asai S, Imagama S. Usefulness of RAPID3 in Assessing Unmet Needs of Patients with Rheumatoid Arthritis in Remission or with Low Disease Activity -a Multicenter Observational Study: T-FLAG Study- [abstract]. Arthritis Rheumatol. 2023; 75 (suppl 9). https://acrabstracts.org/abstract/usefulness-of-rapid3-in-assessing-unmet-needs-of-patients-with-rheumatoid-arthritis-in-remission-or-with-low-disease-activity%e3%80%80-a-multicenter-observational-study-t-flag-study/. Accessed .« Back to ACR Convergence 2023
ACR Meeting Abstracts - https://acrabstracts.org/abstract/usefulness-of-rapid3-in-assessing-unmet-needs-of-patients-with-rheumatoid-arthritis-in-remission-or-with-low-disease-activity%e3%80%80-a-multicenter-observational-study-t-flag-study/